Kashmir Drug Crisis 2026: 13 Lakh Affected, Youth at Risk as Heroin Epidemic Spreads
By: Javid Amin | 23 April 2026
A Crisis in Plain Sight: Kashmir’s Growing Battle with Drugs
Kashmir is confronting one of its most serious internal crises in decades—an escalating drug epidemic that is quietly reshaping its social fabric. With over 13 lakh people affected and more than 1.6 lakh children already using substances, the scale is no longer anecdotal—it is systemic.
What makes this crisis particularly alarming is its demographic profile: young people, especially those aged 17–35, are at the center. The rapid shift from cannabis and prescription drugs to highly addictive opioids like heroin signals a dangerous evolution—one that experts warn could cost the Valley an entire generation if not urgently addressed.
The Scale of the Crisis: A Data-Driven Snapshot
The numbers emerging from Jammu & Kashmir point to a widespread and deepening public health emergency:
- Total substance users: 13–13.5 lakh
- Opioid users: 4.5–5.4 lakh (heroin dominant)
- Children (10–17 years): 1.6 lakh+
- Youth (17–35 years): Most severely affected
Substance Breakdown
- Alcohol: ~3.5 lakh
- Cannabis: ~1.3 lakh
- Sedatives: ~1.5 lakh
The trajectory is particularly concerning: many young users begin with cannabis or sedatives before transitioning to heroin—faster, cheaper, and far more addictive.
What’s Driving the Epidemic?
1. Easy Access to Heroin
Heroin has become more accessible and, in many cases, cheaper than pharmaceutical opioids. Its high potency accelerates dependency, making recovery more difficult.
2. Mental Health Pressures
Years of uncertainty, unemployment, and psychological stress have created a fertile ground for substance abuse. Anxiety and depression often go undiagnosed, pushing youth toward drugs as a coping mechanism.
3. Peer Normalization
Drug use is increasingly normalized in certain social circles. What begins as experimentation quickly escalates into dependency.
4. Stigma and Silence
Families often conceal addiction due to social stigma. This delay in seeking treatment allows substance use to evolve into chronic dependence, complicating recovery.
Social and Health Impact: Families on the Edge
The consequences are visible across households and institutions:
Families Under Siege
Parents are increasingly forced into financial distress—selling assets or taking loans—to fund treatment. Emotional trauma runs deep, often leaving families fractured.
Healthcare System Under Strain
De-addiction centers, particularly in Srinagar, are overwhelmed. High relapse rates indicate gaps in long-term rehabilitation and aftercare.
Rising Disease Risk
Injectable drug use has significantly increased the risk of HIV and hepatitis infections, adding another layer to the public health burden.
Erosion of Community Structures
Kashmir’s traditionally strong family and community systems are weakening under the pressure of addiction, altering long-standing social dynamics.
Government Response: Enforcement vs Rehabilitation
The administration, under the leadership of Manoj Sinha, has launched an aggressive “war on drugs” campaign.
Key Measures
- Demolition of properties linked to drug money
- Cancellation of licences, passports, and Aadhaar of traffickers
- Financial crackdowns and network disruption
The Core Limitation
While enforcement has intensified, experts caution that criminalizing users without parallel rehabilitation risks worsening the crisis. Addiction, by medical definition, is a chronic disorder—not merely a legal violation.
Lessons from Elsewhere: What Works
Kashmir is not the first region to face such a crisis. Proven models offer critical lessons.
🇮🇳 Punjab’s Rehabilitation Model
Punjab’s anti-drug strategy has evolved from enforcement to rehabilitation and reintegration:
- Medication-assisted treatment (buprenorphine, methadone)
- Employment-linked recovery programs
- Education and vocational reintegration
🇵🇹 Portugal’s Health-First Approach
Since 2001, Portugal has treated drug use as a public health issue:
- Decriminalization of personal use
- Dissuasion panels (doctors, psychologists, social workers)
- Significant drop in HIV infections and overdose deaths
🇮🇸 Iceland’s Youth Prevention Strategy
Iceland focused on prevention:
- After-school engagement (sports, arts)
- Strong parental involvement
- Community monitoring
Result: One of the lowest youth substance abuse rates in Europe.
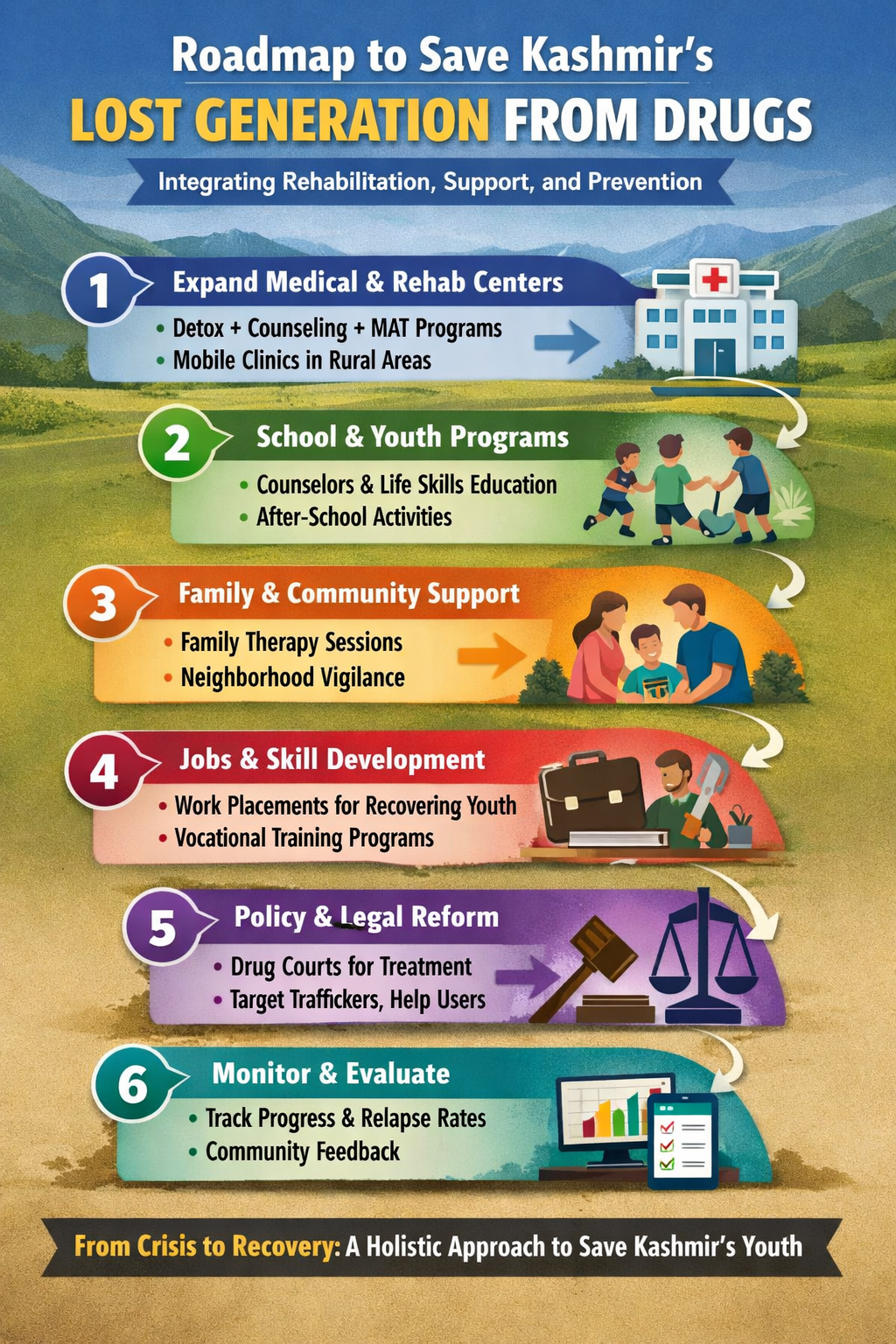
A Six-Step Action Plan for Kashmir
Drawing from these models, Kashmir needs a calibrated, multi-sector response:
Step 1: Expand Medical & Rehabilitation Infrastructure
- Integrated rehab centers combining detox, psychiatric care, and skill-building
- Medication-assisted treatment (MAT) for opioid users
- Mobile clinics to reach rural populations
Step 2: School & Youth Interventions
- Mental health counselors in schools
- Life-skills education and drug awareness
- After-school engagement programs (sports, arts, culture)
Step 3: Family & Community Engagement
- Family therapy programs
- Mohalla-level vigilance committees
- Survivor-led awareness campaigns
Step 4: Employment & Reintegration
- Job guarantees and apprenticeships for recovering youth
- Vocational training (IT, crafts, tourism)
- Microfinance support for affected families
Step 5: Policy & Legal Reform
- Shift from punishment to treatment for users
- Drug courts for non-violent offenders
- Continued strict enforcement against traffickers
Step 6: Monitoring & Transparency
- Real-time data tracking on addiction and recovery
- Public dashboards for accountability
- Continuous policy feedback from communities
Risks if the Crisis Is Not Addressed
- A lost generation trapped in addiction cycles
- Surge in HIV and hepatitis cases
- Long-term social disintegration
- Economic stagnation due to declining youth productivity
The Road Ahead: A Test of Policy and Compassion
Kashmir stands at a critical juncture. The current enforcement-heavy approach has disrupted supply chains, but it has not addressed demand—the deeper psychological and social drivers of addiction.
The real challenge lies in balancing control with care.
If the Valley integrates:
- Punjab’s rehabilitation model
- Portugal’s health-first framework
- Iceland’s prevention strategy
…it can shift from crisis management to long-term recovery.
Conclusion: Saving a Generation Before It’s Too Late
Kashmir’s drug crisis is not just a law-and-order issue—it is a public health emergency, a social crisis, and a generational threat.
The central question is no longer whether the problem exists—it is whether the response will be adequate.
Without a shift toward rehabilitation, mental health support, and community-driven prevention, the Valley risks replacing one form of instability with another—this time from within.


